Serum Free Light Chains And Renal Failure
Free Light Chains Serum Regional Medical Laboratory
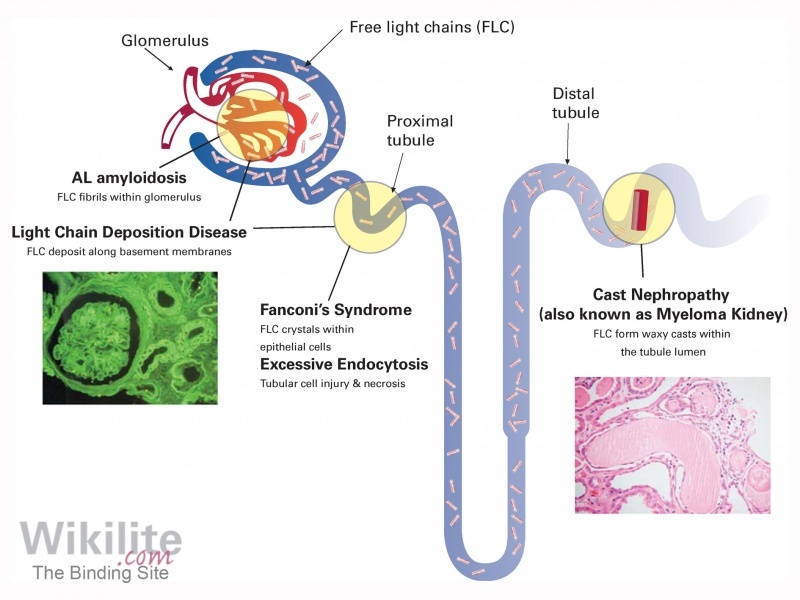
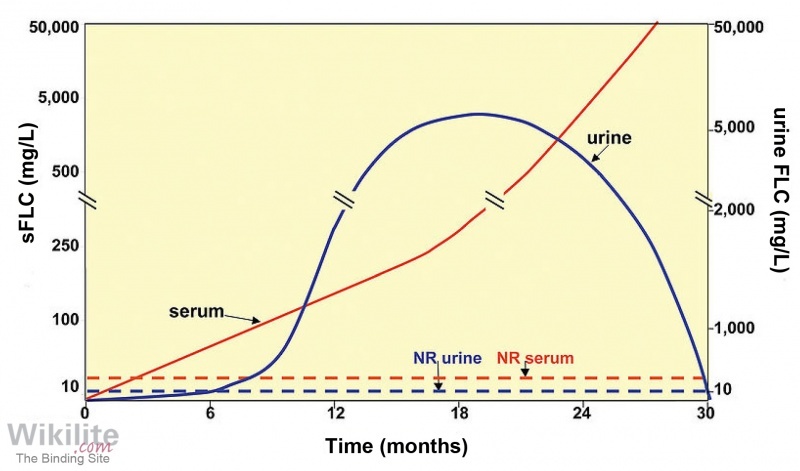
An Overview Of The Kidney And Monoclonal Free Light Chains Wikilite

Serum Free Light Chain Assays Not Total Light Chain Assays Are The Standard Of Care To Assess Monoclonal Gammopathies

Warde Medical Laboratory
Can Serum Free Light Chains Be Used For The Early Diagnosis Of Monoclonal Immunoglobulin Secreting B Cell And Plasma Cell Diseases Full Federal Practitioner
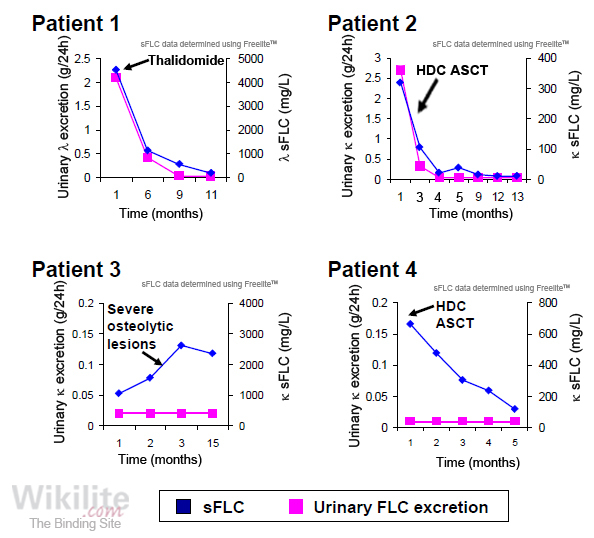
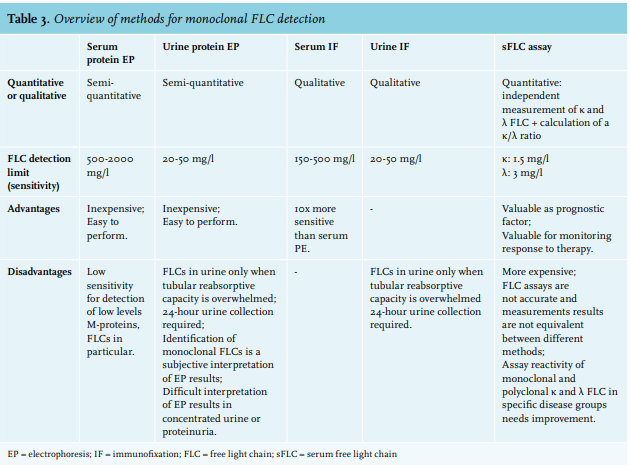
Serum Versus Urine Tests For Free Light Chains Wikilite
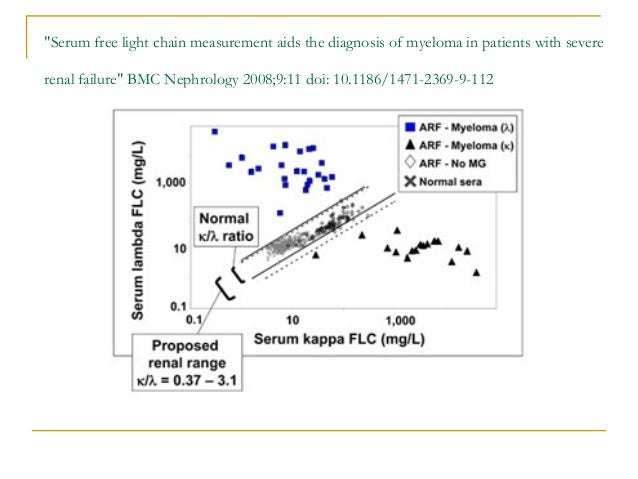
Acute renal failure is observed less frequently 8 30 while chronic kidney disease is quite common 30 60.
Serum free light chains and renal failure.

Comparison Of 2 Serum Free Light Chain Assays In Ckd Patients Kidney International Reports

Serum Free Light Chain Assays Not Total Light Chain Assays Are The Standard Of Care To Assess Monoclonal Gammopathies Sciencedirect

Understanding Free Light Chains Flcs Amyloidosis Patient Information Site

Full Text Polyclonal Free Light Chains Promising New Biomarkers In Inflammatory Cbf
Serum Free Light Chain Assay
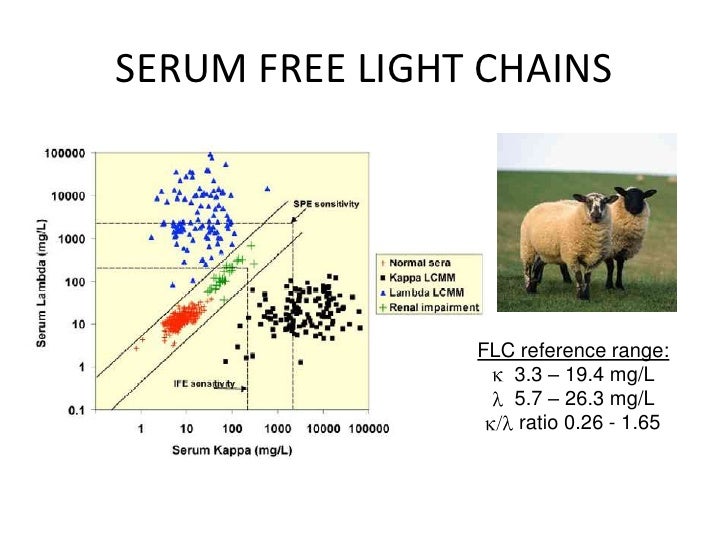
Serum Free Light Chains
Https Alliedhealth Lsuhsc Edu Clinicallaboratory Powerpoint 20for 20clpc Spring 202018 Athas 20revised 20mm 20sp 202018 20b W Pdf

The Association Of Serum Free Light Chains With Mortality And Progression To End Stage Renal Disease In Chronic Kidney Disease Systematic Review And Individual Patient Data Meta Analysis Mayo Clinic Proceedings
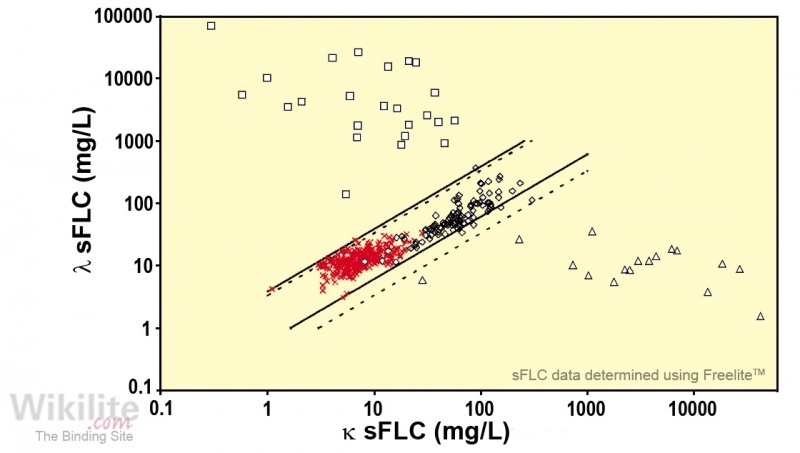
Freelite Reference Intervals Wikilite

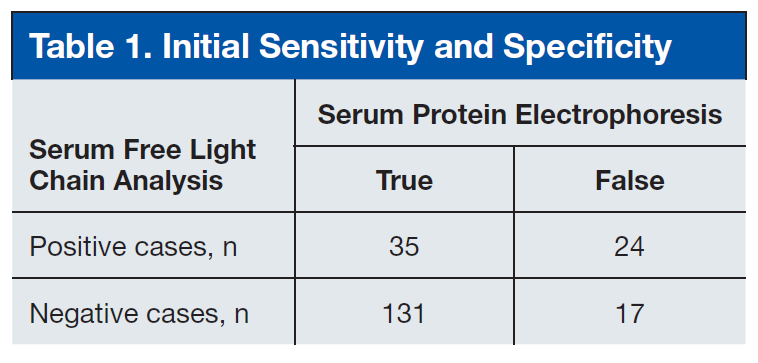
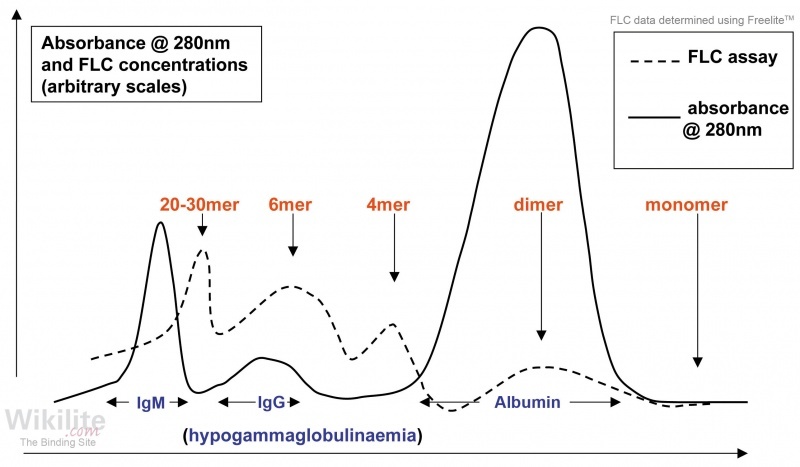
Interpretation Of Serum Protein Electrophoresis And Serum Free Download Scientific Diagram
Https Www Clinlabint Com Fileadmin Pdf Pdf General Serum Free Light Chain Ratio Predicts Outcome In Mgus Pdf
Nonsecretory Multiple Myeloma Wikilite

Serum Free Light Chain Analysis Davids 2010 American Journal Of Hematology Wiley Online Library

Rate And Predictors Of Finding Monoclonal Gammopathy Of Renal Significance Mgrs Lesions On Kidney Biopsy In Patients With Monoclonal Gammopathy American Society Of Nephrology

Is Accuracy Of Serum Free Light Chain Measurement Achievable In Clinical Chemistry And Laboratory Medicine Cclm Volume 54 Issue 6 2016
The Biology Of Immunoglobulins Wikilite

Relevant Investigations In Myeloma 12 Download Table

Pdf Serum Free Light Chain Ratio Is An Independent Risk Factor For Progression In Monoclonal Gammopathy Of Undetermined Significance Mgus
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcteibyhrlxmxbyc7unyjyomvtn7dh7e4qqtpd97kzu Usqp Cau
Comparison Of Serum Free Light Chain And Urine Electrophoresis For The Detection Of The Light Chain Component Of Monoclonal Immunoglobulins In Light Chain And Intact Immunoglobulin Multiple Myeloma Haematologica

Immunoglobulin Light Chain Amyloidosis 2018 Update On Diagnosis Prognosis And Treatment Gertz 2018 American Journal Of Hematology Wiley Online Library
Light Chain Deposition Disease Unc Kidney Center

Full Text Non Secretory Multiple Myeloma From Biology To Clinical Management Ott

Pdf Polyclonal Free Light Chains A Biomarker Of Inflammatory Disease Or Treatment Target Semantic Scholar
Https Www Pennmedicine Org Cancer Media Event 20media 2018 Cancer 11 20november 10th 20focus 20on 20blood 1000 Workshop10 Monoclonal Gammaopathy Ashx

Multiple Myeloma Diagnosis And Treatment American Family Physician
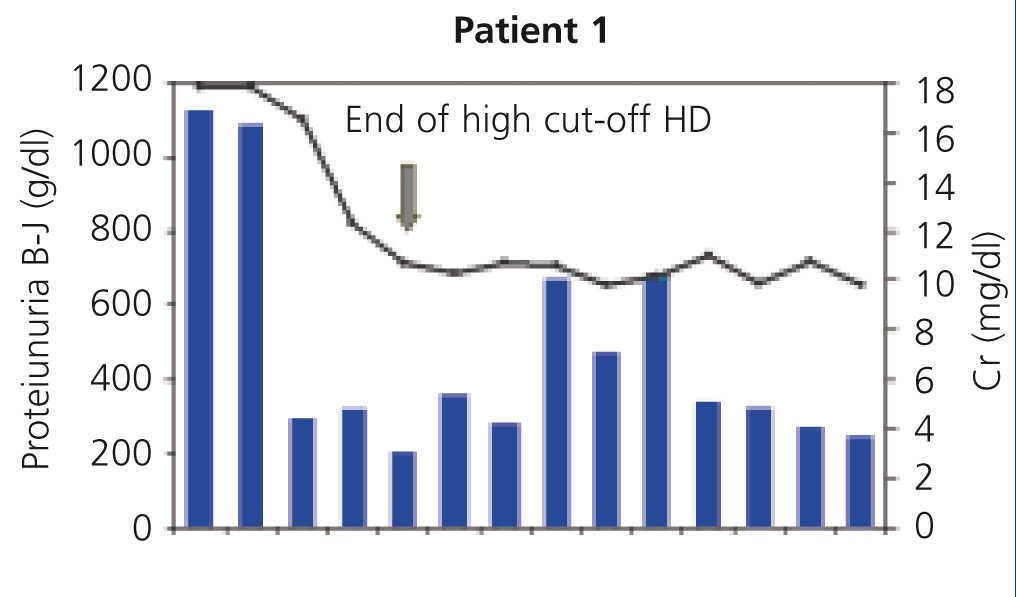
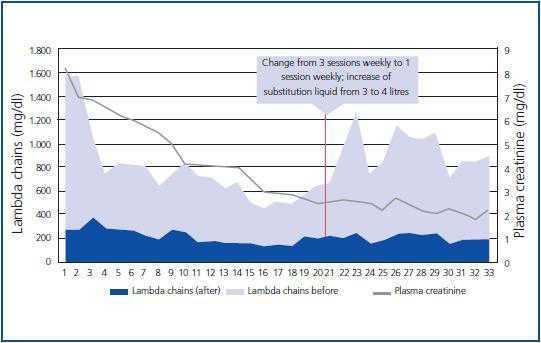
Treatment By Long Haemodialysis Sessions With High Cut Off Filters In Myeloma Cast Nephropathy Our Experience Nefrologia English Edition
Https Www Leicestershospitals Nhs Uk Easysiteweb Getresource Axd Assetid 63843 Type Full Servicetype Attachment

Comparison Of Sebia Free Light Chain Assay With Freelite Assay For The Clinical Management Of Diagnosis Response And Relapse Assessment In Multiple Myeloma Clinical Lymphoma Myeloma And Leukemia
Article Monoclonal Gammopathy Of Renal Significance Mgrs Histopathologic Classification Diagnostic Workup And Therapeutic Options Full Text September 2019 Njm
Plasmapheresis As A Co Treatment In Acute Renal Failure Secondary To Myeloma Kidney Nefrologia English Edition
Pdf Abnormal Serum Free Light Chain Ratio Does Not Always Indicate Monoclonal Gammopathy
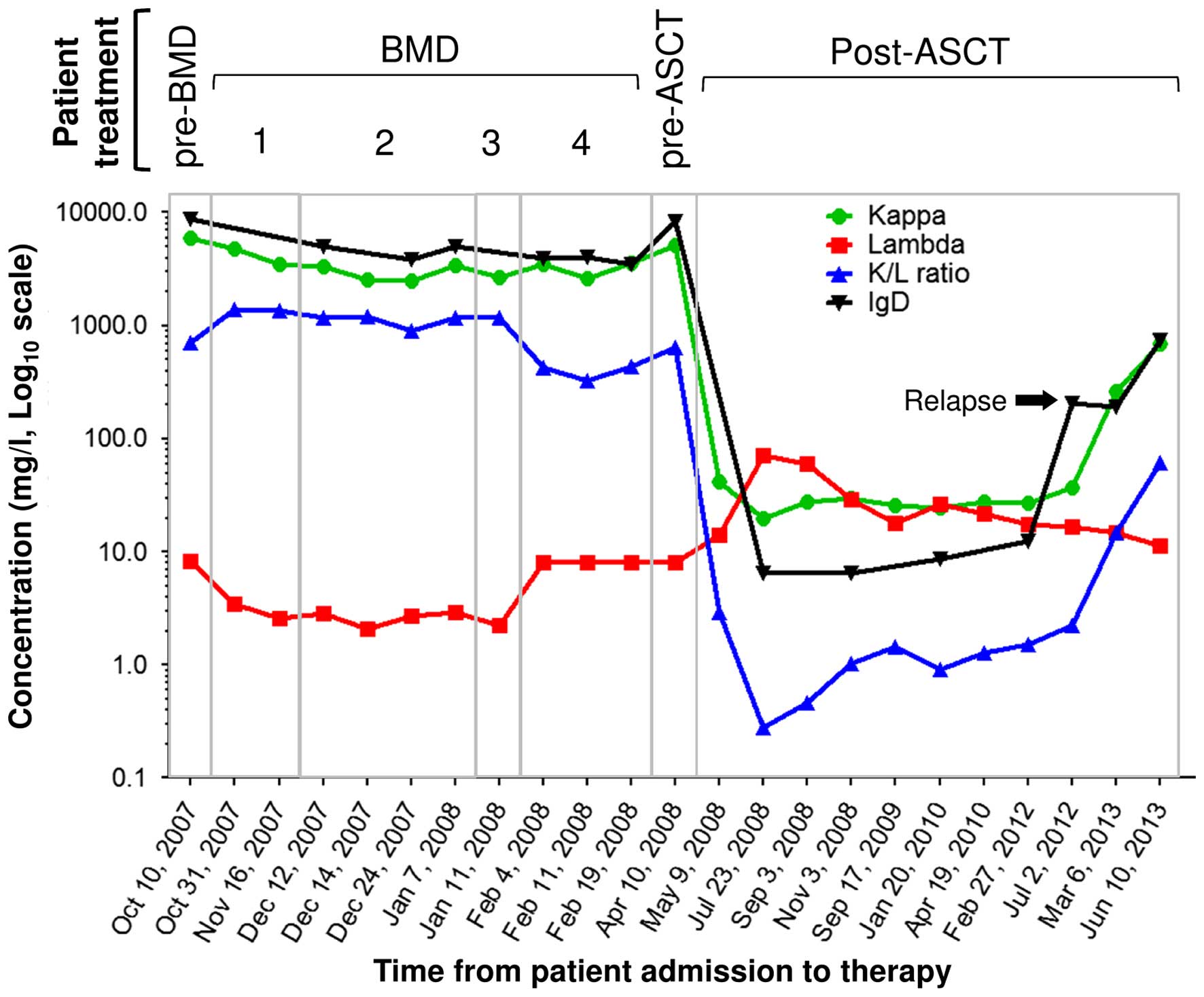
Follow Up Of Igd K Multiple Myeloma By Monitoring Free Light Chains And Total Heavy Chain Igd A Case Report
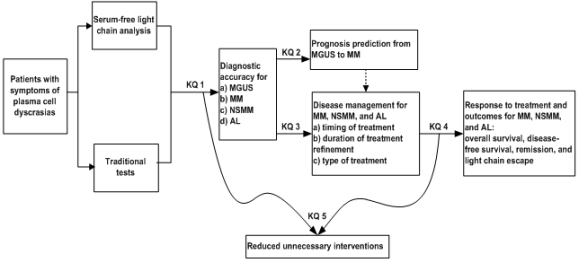
Serum Free Light Chain Analysis For The Diagnosis Management And Prognosis Of Plasma Cell Dyscrasias Effective Health Care Program
Https Effectivehealthcare Ahrq Gov Sites Default Files Pdf Plasma Cell Dyscrasias Sflc Assay Research Pdf

Multiple Myeloma Diagnosis And Treatment American Family Physician
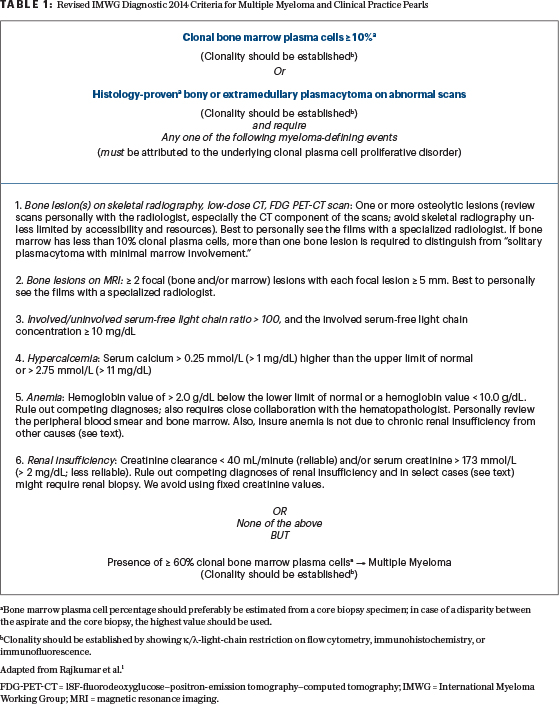
Updated International Myeloma Working Group Criteria Diagnostic Challenges The Asco Post

Paraprotein Related Renal Disease Sciencedirect
Haemodialysis Using High Cut Off Dialysers For Treating Acute Renal Failure In Multiple Myeloma Nefrologia English Edition

Free Light Chains And Autoimmunity Sciencedirect
A Diagram Of Intact Immunoglobulin Showing The Structure Of The Heavy Download Scientific Diagram

72 Year Old Man With Acute Kidney Injury Hypercalcemia And Metastatic Prostate Cancer
View Of Bortezomib Maintenance For The Treatment Of Monoclonal Gammopathy Of Renal Significance Mediterranean Journal Of Hematology And Infectious Diseases
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcteibyhrlxmxbyc7unyjyomvtn7dh7e4qqtpd97kzu Usqp Cau
Source : pinterest.com
